SEMI-CLOSED HEMORRHOIDECTOMY BY CIRCULAR STAPLING Download in PDF
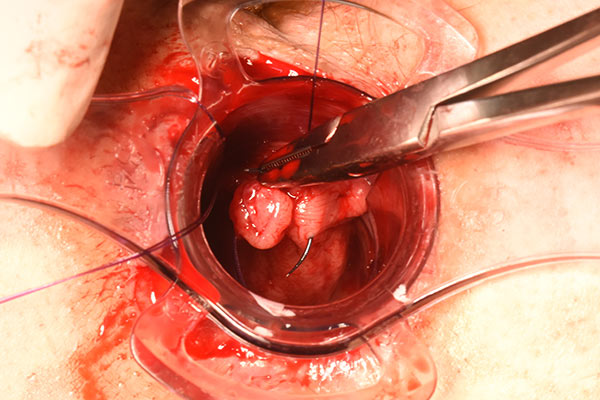
This procedure leaves in place 3 open incisions on the edge of the anal canal by\stapling the rectal mucous membrane allowing it to be fixed to the lower rectum and thus at the same time performing a 3 tied pedicle excision during the first phase of the Milligan and Morgan operation .
These two combined procedures result in a semi-closed hemorrhoidectomy (3 mini open cut drains remain) I stress the fact that you must first perform a Milligan and Morgan procedure and then staple and not staple then excise some marisca as is frequently practised in France nowadays.
Removal of external and internal hemorrhoids and the mucous prolapse during the same surgical operation,
Shrinking external cuts along with the tightening of the anal canal,
Removal of ligated pedicles,
The removal of pedicles results in the absence of necrotic oozing of these pedicles (one has only to look at the appearance of the anal canal during a return to surgery for secondaty bleeding for example on day 10),
Decreased oozing results in less postoperative pain and a shorter duration of this pain. The pain experienced is similar to that of the Longo procedure,
Faster healing time (around 18 days),
Lower risk of secondary bleeding when scabs fall off on day 10 after surgery,
No post-operative marisca as stapling the bridges towards the inside of the anal canal causes tightening.
Decreasing of the surface of the intra-canalaire wounds due to a reduction and a binding of the rectale membrane,
Calibration of the anal canal by the circular stapling leading to a decreasing of the postoperative stenosis,
Corection of an anterior rectocele by stapling.
II) Disadvantages :
No single technique is ever completely free from disadvantages or complications : Immediate morbidity identical to the other techniques,
Difficulty of the technique : at the time of stapling, during the second part of the operation after having performed a Milligan and Morgan procedure (the excision of a group of hemorrhoids),
The need to have sufficient experience with the basics of Longo Hernorrhoidopexy prion to performing this combined semiclosed technique, (Milligan and Morgan technique),
The systematic use of a stapler to perform this technique which naturally leads to an increase in the cost of the procedure,
The risk of stenosis increases if the stapling done in the second phase goes too deep taking with it ; the muscularis-care must therefore be taken to ensure that only the supedicial mucosa is perforated
Conclusion
Technique which is avalable in around 90% of the hemorrhoidectomy whatever the level of the prolapsus,
The postoperative consequence are more simple with a fastest healing (average of 18 days),
After the day 10, a decreasing of the postoperative pain,
Increasing of the pain due to the hemorrhoidopexy but a clear decreasing of the pain thanks to the Milligan and Morgan technique with or without anoplasty,
This technique needs a kind of apprenticeship (It is needed around 20 procedures).
Actually, we have realized 6700 sugeries with this semiclosed technique from December 2008. On 100 hemorrhoidectomies :